Best Gallstone Operation in Pune
Best Gallstone Operation in Pune
![]() Painless & Minimally Invasive
Painless & Minimally Invasive
![]() Safe & Effective
Safe & Effective
![]() Best Surgeons
Best Surgeons
![]() Surgery Today, Pay Later
Surgery Today, Pay Later
100+
JCI & NABH Hospitals
1,500+
Expert Doctors
8,000+
Happy Patients

Risks of Delayed Gallstone Treatment
- Blockage & Acute Inflammation
- Severe Jaundice
- Obstruction of Gallstones in Bile Duct
- Spread of Infection & Perforation
- Death of Gallbladder Tissue
Our Top Doctors

Dr Priyesh S Halgaonkar
Laparoscopic, and General Surgeon
10 Years
Experience
99%
Positive Reviews
59 Patients already consulted this week

Dr Ankit Potdar
Laparoscopic and General Surgeon
11 Years
Experience
100%
Positive Reviews
56 Patients already consulted this week

Dr Ashish Kale
General Surgeon and Minimal Access Surgeon
10 Years
Experience
99%
Positive Reviews
32 Patients already consulted this week

Dr Ajay Dilip Devershi
General Surgeon
12 Years
Experience
98%
Positive Reviews
35 Patients already consulted this week

Dr Harsh Sheth
General Surgeon, Laparoscopic and Bariatric Surgeon
12 Years
Experience
100%
Positive Reviews
31 Patients already consulted this week
Treatment Cost Depends On
Type of
Procedure
Severity of
the Disease
Past Medical
Condition
Contact
for exact cost



Why Choose HexaHealth
 Expert Experienced Surgeons
Expert Experienced Surgeons
Top NABH Hospitals
Personal Care Assistance
Insurance Approvals
No Cost EMI
What our Patients Say
Reviews
4.8
(3,222 Reviews)
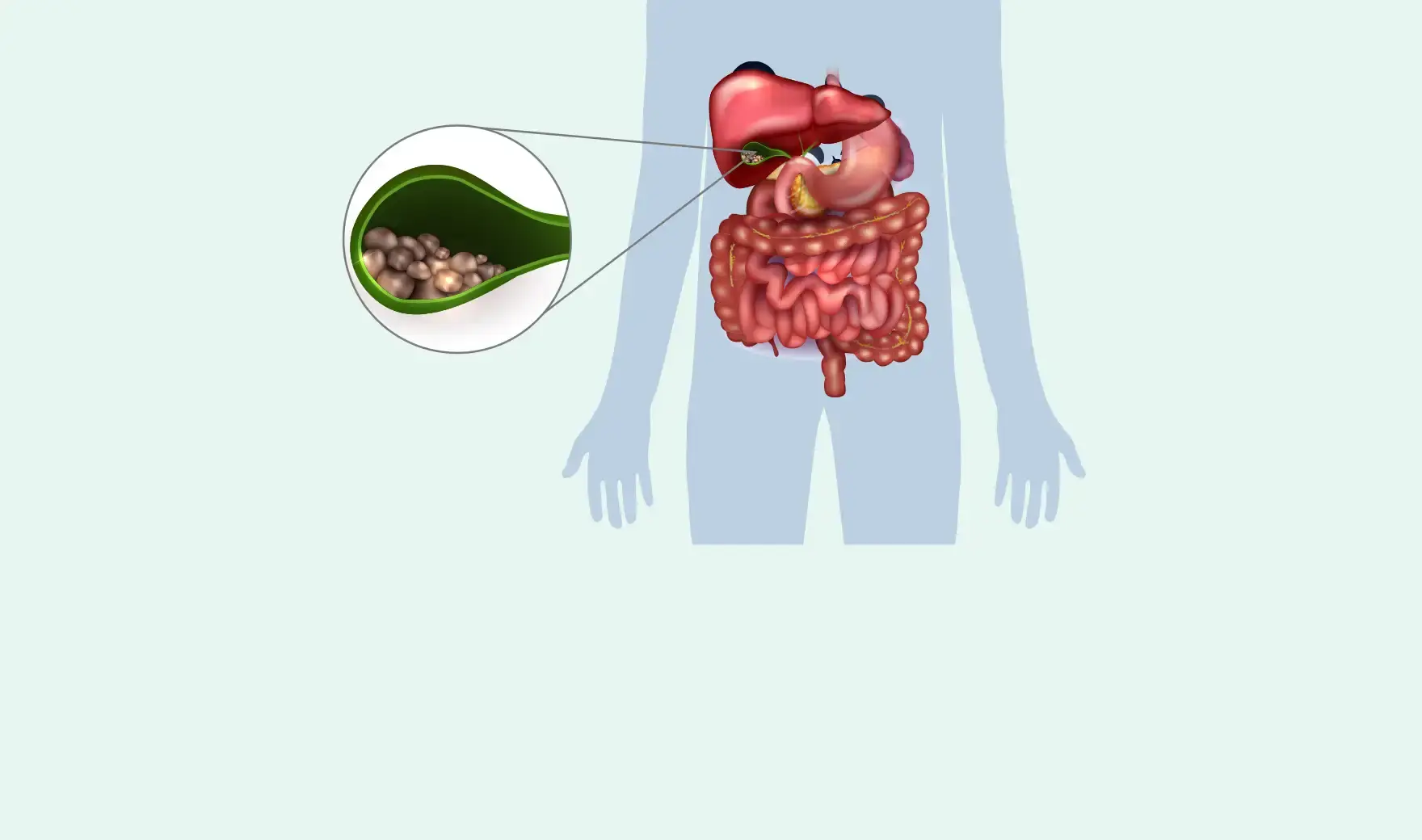
What are Gallstones?
Gallstones or Choleliths are hardened deposits of the digestive juice or bile found in the Gallbladder or Bile duct. They can be made of excess bilirubin, salts or cholesterol. The formation of gallstones in the gallbladder is termed Cholelithiasis.

Frequently Asked Questions
Can you live without a gallbladder?
Yes, one can have a perfectly everyday life without a gallbladder. Your liver will still produce enough bile even without a gallbladder, but instead of bile being stored in the gallbladder, it will drip bile straight into the small intestine. Hence, most foods can still be digested, but oily or high-fibre food becomes harder to digest at times, resulting in gas, bloating, or diarrhoea.
Can we remove gallstones without removing the gallbladder?
Yes, gallstones can be removed without removing the gallbladder. Certain medications help to dissolve stones if the size is small. Endoscopic Retrograde Cholangiopancreatography (ERCP) is a procedure wherein the gallbladder is not removed; instead, any stones in the common bile duct (CBD) are removed using an endoscope.
What happens if a gallstone is detected during pregnancy?
The risk of having gallstones is higher in pregnant females due to elevated hormones. If a gallstone is detected incidentally while doing an ultrasound, then one should not rush to get treated at that time. In the first trimester of pregnancy, the baby's body is under formation. Any medications or drugs needed to perform the surgery can pose a greater risk of developing congenital anomalies. If the patient has recurrent attacks & is not responding to medicines, then surgery can be performed in the second trimester as this is the safest & least risky time. During the third trimester, it is encouraged to postpone surgery until after delivery since the growing uterus can make it difficult to do surgery & even pose a risk for preterm labour.
Is laparoscopic gallstone treatment safe & effective?
Yes, it is with the following benefits:
- Minimally invasive procedure
- Smaller incisions less than 1cm
- Stitchless & Painless
- Next-day discharge
- Minimal blood loss
- No or minimal risk of complications
- Bed rest only for 2-3 days
- High success rate with no reoccurrence
- Recovery is quick & smooth
Does Insurance cover treatment for gallstones?
Yes, all health insurance plans cover treatment for gallstones, especially when it is medically necessary. Our team facilitates paperwork on your behalf, ensuring smooth approval & a cashless facility. Contact HexaHealth for a simple cashless & hassle-free experience.
What is the cost of gallstone removal surgery?
It is variable, considering the size & location of gallstone, technique, open or laparoscopic or ERCP, consumables, patient's medical condition based on age & other health factors, etc. Contact HexaHealth for price transparency.